The 3 Faces of Elbow Dysplasia
Elbow dysplasia is a general term used to identify an inherited polygenic disease in the elbow. Three specific etiologies make up this disease and they can occur independently or in conjunction with one another. These etiologies include:
- Pathology involving the medial coronoid of the ulna (FCP)
- Osteochondritis of the medial humeral condyle in the elbow joint (OCD)
- Ununited anconeal process (UAP)
Recognizing the Signs
Studies have shown the inherited polygenic traits causing these etiologies are independent of one another. Clinical signs involve lameness which may remain subtle for long periods of time. No one can predict at what age lameness will occur in a dog due to a large number of genetic and environmental factors such as degree of severity of changes, rate of weight gain, amount of exercise, etc.. Subtle changes in gait may be characterized by excessive inward deviation of the paw which raises the outside of the paw so that it receives less weight and distributes more mechanical weight on the outside (lateral) aspect of the elbow joint away from the lesions located on the inside of the joint. Range of motion in the elbow is also decreased.
FCP and UAP
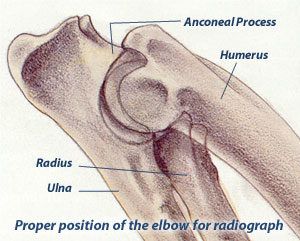
Elbow dysplasia in dogs has multiple inherited etiologies which may occur singularly or in combination. These etiologies include fragmented medial coronoid (FCP) of the ulna, osteochondritis of the medial humeral condyle and ununited anconeal process (UAP). The most sensitive view used to diagnose secondary degenerative changes in the elbow joint is an extreme flexed mediolateral view of the elbow which is required by the OFA and recommended by the International Elbow Working Group. Veterinary radiologists are most interested in the appearance of the anconeal process of the ulna.
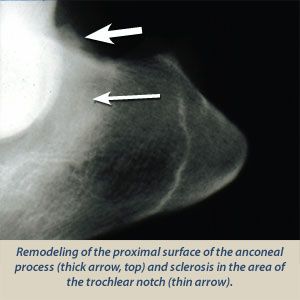
When there is instability of the elbow joint due to elbow dysplasia in a dog, one of the most sensitive radiographic findings is new bone proliferation (osteophytes) on the anconeal process of the ulna associated with secondary developmental degenerative joint disease.
Identifying the Condition
Bone proliferation can be very subtle to visualize in some dogs. Other arthritic findings such as sclerosis in the area of the trochlear notch of the ulna and bone spurs at joint edges are also reported. If fragmentation of the medial coronoid only involves the cartilage, it may not be seen radiographically but occasionally if the bone is also fragmented, it can be visualized as a separate calcific opacity superimposed over the radius.
Explanation of Elbow Grades
For elbow dysplasia evaluations for dogs, there are no grades for a radiographically normal elbow. The only grades involved are for abnormal elbows with radiographic changes associated with secondary degenerative joint disease. Like the hip certification, the OFA will not certify a normal elbow until the dog is 2 years of age. The OFA also accepts preliminary elbow radiographs. To date, there are no long-term studies for preliminary elbow examinations like there are for hips; however, preliminary screening for elbows along with hips can also provide valuable information to the breeder.
- Grade I Elbow Dysplasia: Minimal bone change along anconeal process of ulna (less than 2mm).
- Grade II Elbow Dysplasia: Additional bone proliferation along anconeal process (2-5 mm) and subchondral bone changes (trochlear notch sclerosis).
- Grade III Elbow Dysplasia: Well developed degenerative joint disease with bone proliferation along anconeal process being greater than 5 mm.
Radiographic Elbow Views
The International Elbow Working Group (IEWG), a consortium of experts from around the world was founded in 1989 to lower the incidence of elbow dysplasia by coordinating worldwide efforts. The diagnosis of elbow dysplasia is based on the presence of degenerative joint disease/osteoarthritis which results from an ununited anconeal process, osteochondrosis or a fragmented medial coronoid process. The OFA started its elbow database in 1990 using a modified protocol of the IEWG. For cost effectiveness and mass screening, the OFA requires the extreme flexed medial to lateral view of each elbow. Inclusion of additional views such as the neutral medial to lateral, cranial caudal or preferably the cranial caudal 10-15 degree lateral to medial oblique can also be submitted and will be evaluated.
In instances where the owner is requesting a re-evaluation of the elbows or if the dog is experiencing lameness it is recommended that the cranial caudal 10 to 15 degree lateral to medial oblique view accompany the required extreme flexed medial-lateral view.